I’m a consultant who, amongst other things, helps organizations increase their organizational productivity and employee engagement through process improvements. In other words, I’m one of those nerds who, while waiting in line, can’t help but see inefficiencies and devise ways (in my head) for how to improve it. I do this while waiting in line anywhere: at airports, supermarkets, amusement parks and, more recently, while waiting to be tested for the Covid-19 virus.
It took a total of 2 hours and 20 mins, not counting the commute to and from the hockey arena that had been commandeered as a testing center. This was a few weeks ago. Currently, with a new surge in cases in Ottawa, where I live, the demand for tests has shot through the roof and the wait times are so long that people are being turned away. If you’re a person of some celebrity, the media might even care: recently, there have been highly publicized stories of people like Erin O’Toole, the leader of the Conservative Party of Canada, waiting for hours and hours.
But it’s not just MPs who need to get tested (O’Toole tested positive, by the way). Ordinary people who have symptoms or who have come into close contact with an infected person need to get tested too. Both the anti-maskers and the strict lockdown camps can agree on this. We can only isolate the healthy from the sick if we know who’s sick and who’s not. But to encourage people to get tested—indeed, to get people to do almost anything– we need to make it easy for them to do so. Long lineups are, quite obviously, not helping. But there’s something we can do to alleviate them.
The process for getting tested has three steps to it: 1. registration, where they check your health card and enter your basic data into their database; 2. an interview with a nurse, who gathers some info about why you’re getting tested; and 3. the test itself. The steps are fairly routine and the amount of time patients spend at each step does not vary much. In total, the process takes about 25 minutes. I’ve made a simplified diagram in Figure 1.
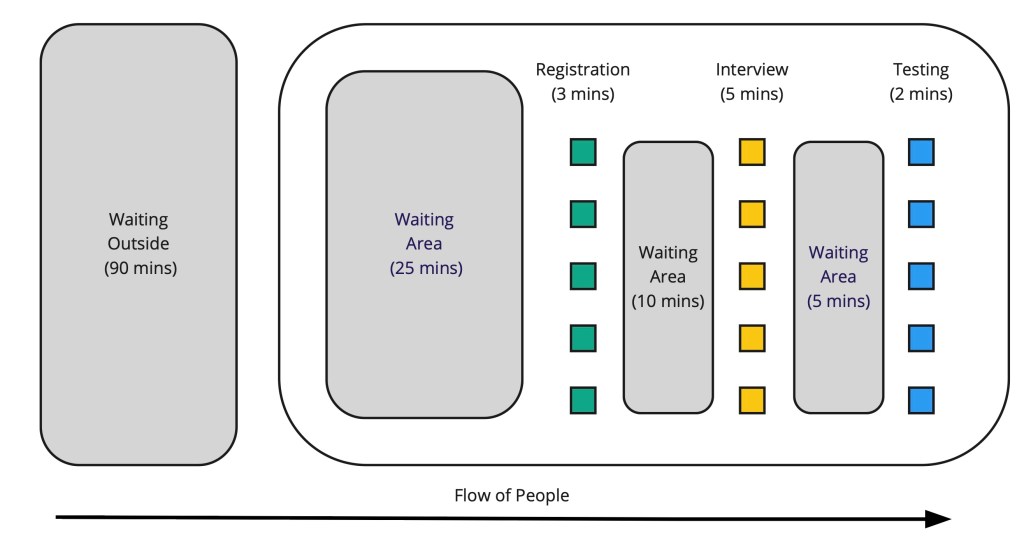
The fundamental problem behind the wait times is the imbalance in the processing times at each of the three steps. In my diagram, the times for the three steps are 3, 5, and 2 minutes (which are purely estimates—use a stopwatch if you’re actually going to try this). To be clear: I’m not suggesting the nurses doing the interviews speed up and while the testers slow down so that we get an average of 3.33 minutes per process step.
There is another, and much better, way to speed up a process without making anyone cut corners or work faster or harder. Nor does it involve any additional costs, hiring extra people or introducing new technology.
The simple way to remedy this situation is to simply move the existing staff to the work. How? It involves some simple math, performed in three simple steps.
First, add up all of the average processing times for each of the separate three steps, which in my example amounts to 3+5+2 = 10 minutes. Don’t count the patient waiting times in between the steps, only the work activity time of the healthcare workers. Secondly, divide the sum of the processing times (10 minutes) by the total number of employees available. In my diagram, I’ve represented one employee by a square: there are 5 employees at each process step for a total of 15 workers. So now, following this simple equation, you have 10/15 or .66 of a minute (40 seconds).
The third step is to go back to the original processing times for each individual step (3, 5, and 2 minutes) and divide each by .66 minutes. This will tell you the optimal number of healthcare workers you need to allocated to each step, which turns out to be 4.5, 7.5, and 3.0, respectively. Note that it still adds up to 15 people— we’re not aiming to increase the number of workers, only to optimize the existing, “as-is” process without extra labour.
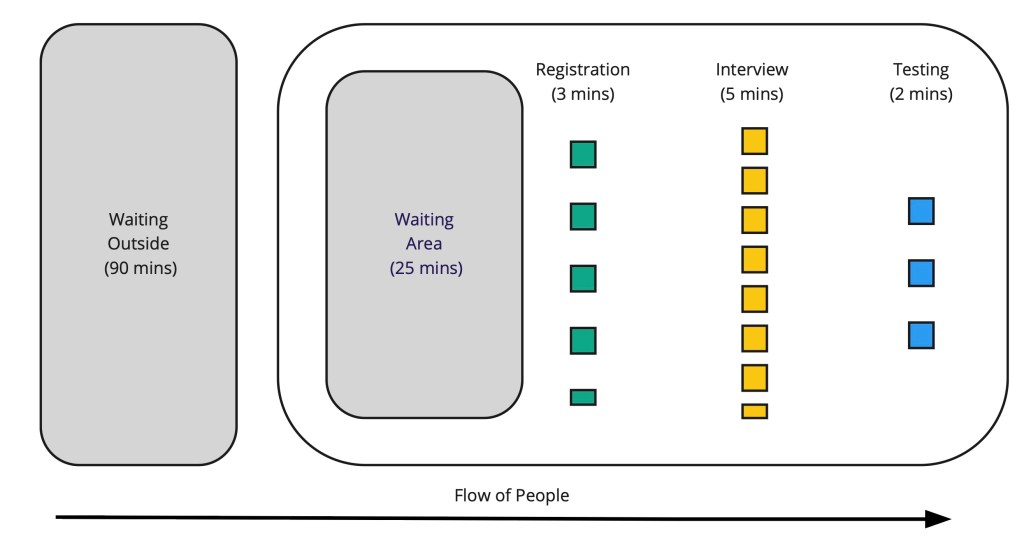
Now, if you could allocate exactly 4.5, 7.5, and 3 people to each process, the time it takes for a patient to move from starting registration to completing the test will now be 10 minutes, not 25 minutes. That’s a 60% reduction in processing time, and that’s pretty amazing, if you think about it. We’ve cut the processing time by more than half without adding any extra people, without asking anyone to work harder or faster, and without adding any new technology. This means that if there are 100 people in line for a test, it will now take the 100th person in line just over an hour (66 minutes) of waiting to get tested, whereas in the current arrangement it would take over two and a half hours (167 minutes). How did we do this? Basically, we just obliterated the waiting time between the three process steps, as you can see in Figure 2.
“But life’s not that simple!”, I can hear you objecting already. And, yes, it’s true, life’s not that perfectly neat and tidy. You can’t easily divide up an employee’s labour into halves. It takes time for patients to physically move from one step to the next. The skillset required to do registration (data entry) is different from that required to do interviews, which is different again from that of administering the test. All of these reasons and more for why it potentially “won’t work” are perfectly welcome.
Why welcome? Because they make the context dynamic—just like any workplace—and it requires those involved in the process—our smart, brave and tireless healthcare workers– to use their creativity and ingenuity to respond to changing conditions and challenges. And this is a big part of what makes any job interesting: using one’s creative ideas to improve and innovate their work on the fly. In this case, the work is driven by the purpose of better public health.
But one has to start by redesigning the process according to the simple mathematical steps I’ve outlined above, and then adapt and adjust, constantly and forever. Only before you start adapting and adjusting, you have to do one more crucial thing: move the process steps physically closer together. No closer than 6 feet, of course, but far closer than they are spaced today (in hockey rink terms, the currently layout starts near the blue line and ends at the opposing goal line). Leave as little room as safely possible for people to wait in between steps. I know that sounds counter-intuitive, but the reason is to make problems visible to all. Problems that are visible have a way of eliciting creative solutions.
When I was there, there was a small army of people in full PPE rushing to wipe down chairs with sanitizer and disinfectant after every new person sat in one. Every patient sat in no fewer than five different chairs as they went through the process, and that required five separate disinfecting routines per patient. That’s a lot of labour that could be used more productively elsewhere (e.g. registering, interviewing or testing). Eliminating the waiting areas in between processes means no waiting and no more than one chair per patient to disinfect. Have people take a disinfected folding chair at the beginning of the process and have them carry or drag it with them through all three steps (which are now separated by only 6 feet).
The result is something like Figure 3.

Now we’ve got 4 people in registration, 8 in interviewing, and 3 in testing. Further, the workers in registration and interviewing will be arranged in clusters (you can call them “cells” or “pods” if it sounds better) of 3 people, all 6 feet apart, of course, and the registration process will feed the interviewing process. The patient will only move forward from registration when one of the two interviewers is free. Similarly, patients can only move forward from interviews to testing once one of the three testing stations is free.
The result is that sometimes some of the workers (and patients) will be sitting around briefly, waiting for the next step to open up. So long as it is a short delay…so what? These workers fully deserve additional breaks on top of their officially scheduled ones. If the underutilization is prolonged and impacting the overall processing time (which should realistically be around 12 minutes, allowing for up to two minutes waiting in between steps), then recalculate using the three steps and readjust the ratios until the waiting time for patients shrinks.
A bonus feature of this arrangement is that a far greater area of the arena can be devoted to line ups. Given the nature of Ottawa’s winters, having to line up outside is not likely to entice more people to get tested. The clustering is a far more productive use of space.
But the best part of this model is that it is adaptable. The number of staff available will vary from shift to shift and from day to day. And in these cases, all you have to do is recalculate and rebalance using the three simple math steps that I’ll repeat here:
1. Sum the total processing time across all the three steps.
2. Divide this sum from Step 1 by the number of available workers.
3. Divide the processing times at each separate step by the number from Step 2, round to the nearest integer, and allocate that number of staff to each process step accordingly.
What about reducing the processing times? Yes, of course! A whole raft of other improvements can be made, such as supplementing central testing facilities with testing at local pharmacies (a plan that’s in progress, apparently). Schedule visits online. Extend the hours. Expand drive through testing. Devise “phone booth” testing, as they did in South Korea. Use different tests (e.g. with blood or saliva) instead of the unpleasant nasopharyngeal swab, if they are reliable and quicker and easier. Add capacity to the labs to get the results sooner. There is no end to the opportunity for improvements to be made. And, as the processing times change, all you have to do is recalculate according to the three steps and adjust. Health authorities do not have to spend more money. They have to spend creativity.
Lastly, in case you’re wondering, it took 36 hours for me to receive my results through an app on my phone. I tested negative.
